
Mark Twain said, “Eat a live frog first thing in the morning and nothing worse will happen to you the rest of the day.” When I first read this quote, I thought it was just a bit of silliness and good fun, but I read once that it meant that you should tackle your most dreaded task first. This is good advice for often dreaded tasks are not as difficult as we feared. We just need to get started.
My long-range calendar is kept in Outlook, but I do not use Outlook to keep track of what I need to do today. I have often found myself ranging over the hospital so I would not have immediate access to my desktop computer. I also want to be able to talk on my phone and look at my schedule at the same time. So, to prepare for tomorrow, I pull out an unlined 3 x 5 index file card. Orienting it in a portrait layout, I write the day of the week and the date at the top. Below this I write in my known schedule for the day. If meetings are back to back, I write them with no space in between. If I have time between meetings, I leave space to write in commitments that will be made that day.
If you have a job with clear and regular boundaries between work and personal time, it may be practical to keep two separate calendars. But those of us in leadership, especially hospital leadership, find the boundary between work and personal time to be very fluid. We may have to come in early one day to meet with the surgeons and the next day stay a couple of hours into the evening for hospital committee meetings. Under these circumstances, it is critical that there only be one calendar on which is kept all work and personal commitments. One of Steve Jobs’ daughters understood this principle well. When her father would commit to spend time with her, she would call his secretary and have her add the event to his calendar.
If someone helps you with your schedule, it may be necessary to give them access to your Outlook calendar so that they can schedule meetings for you. If you feel you need privacy, it is possible to add things to your Outlook calendar such that others can see that the time is blocked but cannot see how you labeled the event.
On the backside of the 3 x 5 index file card, I write my “to do” list. These are things that I want to get done in my open time between meetings. As things are completed, I cross them off. Anything uncompleted by the end of the day, can be added to the next day’s “to do” list. For me there is always something to carry over on my “to do” list to the next day for I am a very ambitious “to do” list writer.
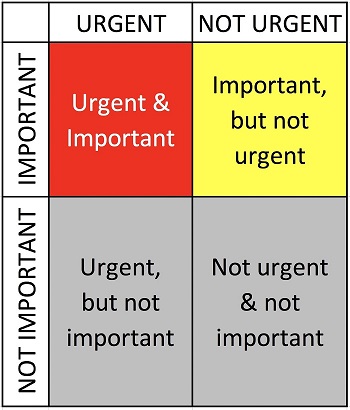
So how do we prioritize our “to do” list? We can begin by looking at our list in terms of a Johari window. Tasks can be divided into urgent & important, not urgent & important, urgent & not important and not urgent & not important. We must be careful about how we characterize our tasks. We may think that something is not important, but we can make a serious mistake if we decide that a task in unimportant while our boss thinks it is extremely important. We can lighten our load and focus our energies by removing things that are truly not important from our “to do” list. In the short term we must tackle urgent and important tasks, but in the long run we want to complete our tasks that are important while they are still not urgent.
There is merit in quickly knocking out easy tasks that are important, but we must not allow our sense of accomplishment to excuse us from tackling difficult tasks that we need to get done.
No is a word that I do not like to say to my superiors. I was hired to make things happen and to get things done. I was hired to be a solution to problems. When given a problem, I want to serve, I want to help. This can result in overloading my schedule. After starting a job as a physician leader, I was invited to sit on several committees. Early on I was given advice by one of my bosses that I should limit the number of committees that I sat on. So, I asked him to give me a number of how many committees he thought I should be on. As I accepted these committee assignments, I let them know that I had a limited number of committees that I could be on and that I might have to step down from their committee if the hospital needed me somewhere else. I had the advantage that I oversaw 22 physicians and four nurse practitioners who each needed to sit on at least two hospital committees. With so many providers needing committees, I struggled to find places for them all. When I needed to step down from one committee to take on a more important assignment, I was always able to replace myself with one of these providers.
Stephen Covey listed “sharpen your saw” as one the seven habits of highly successful people. A carpenter who only saws and never takes the time to sharpen his blade will be very unproductive sawing with a dull blade. We must take time to plan, prioritize and organize our work. This gives our work focus and power. We feel more effective, because we are more effective, and that sense of accomplishment brings joy and meaning to our work.
Connect with us on LinkedIn, join our Active Network Program and look at the other areas of connection we offer.


















